Bladder cancer is the 2nd most common cancer of the urinary system, after prostate cancer. In men, it is 4 times more common than in women. Due to high risk of recurrence, regular lifelong review with ultrasound and cystoscopy is necessary. In aggressive stages random biopsies and CT scan are needed.
There is no clear etiology. However, there are some risk factors that increase the chances of its occurrence such as:
Painless gross or microscopic hematuria is the most common symptom of the disease. Remarkable is the fact that even a single episode of hematuria, without any recurrence, can hide bladder cancer. Other less common symptoms of the disease are painful urination, frequency, urgency, weakness and weight loss.
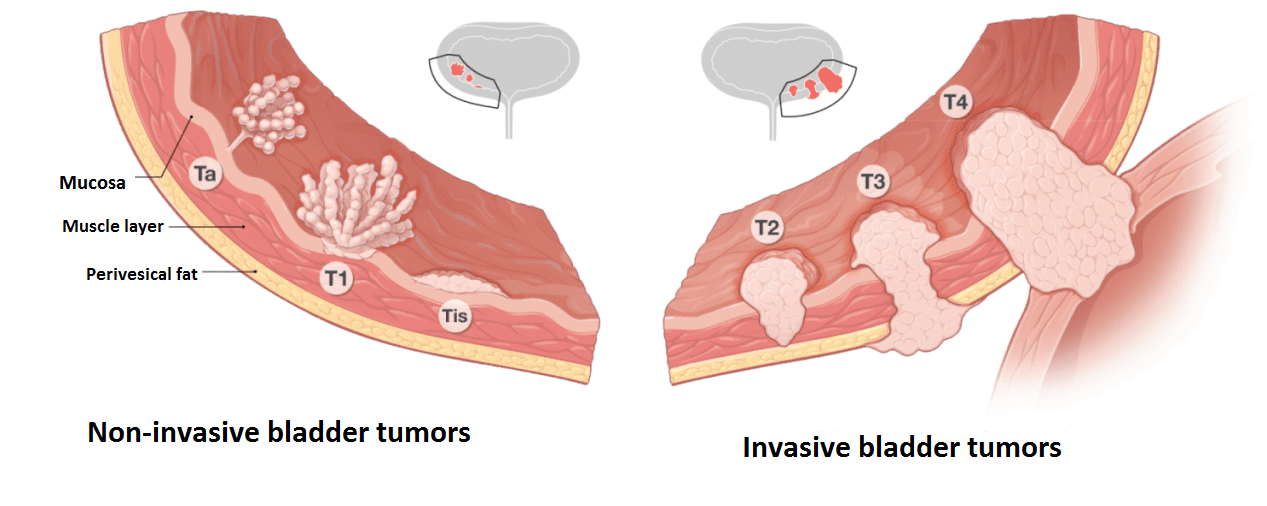
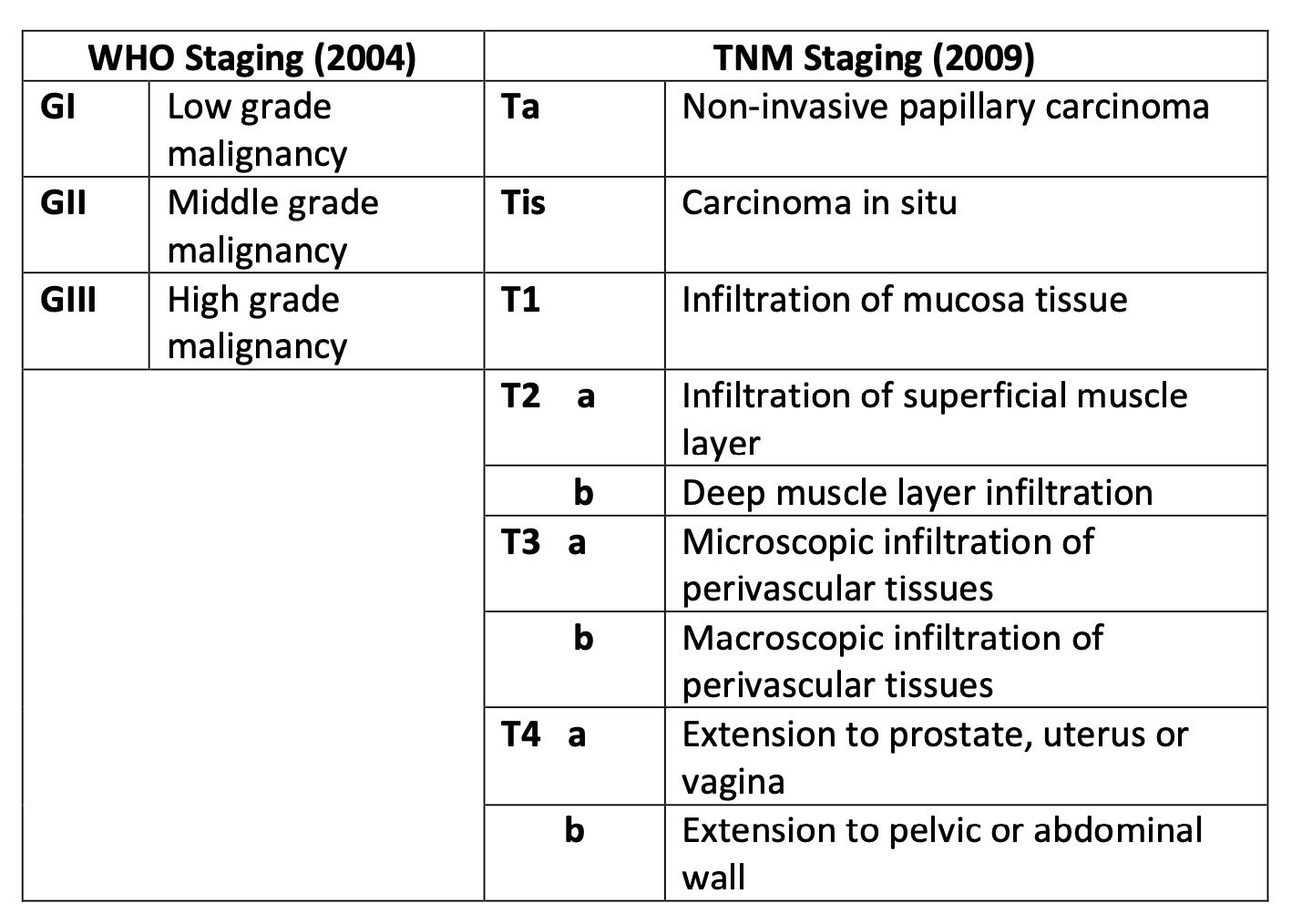
Diagnosis is made by cystoscopy and Bladder Biopsy. If the disease is diagnosed, it is very important to perform staging with CT scan and bone scanning to investigate metastatic disease. Bladder cancer is staged as:
The type of treatment depends on the stage of the disease and the general condition of health of the patient.